Back in the saddle, day 1
I have six months to train for the August deadline of the 100 mile Prudential Cycle ride and that means I need six months to prepare.
Today was taking that first bite from the elephant and I covered 25.7 in two sets: one of 20.5 miles and then a return home of 5.2 miles. In total the average is 10.8mph.
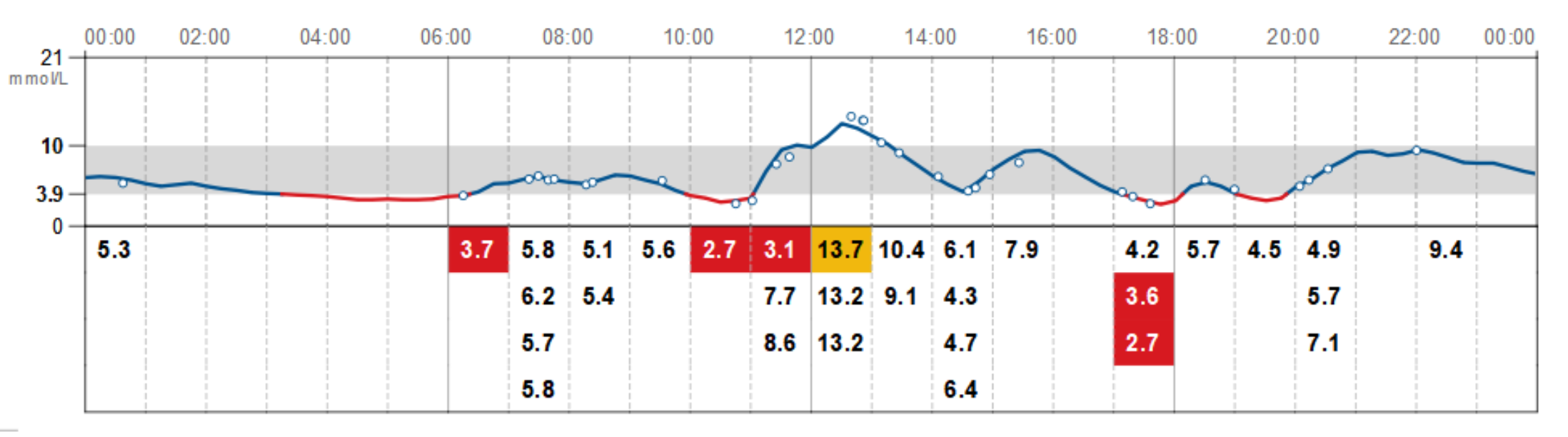
The sun was shining, my blood sugar was not behaving itself but actually this was an interesting view on what cycling with high blood sugar would be like with a safety net (son at home for half-term and able to drive).
Getting ready to head out did not take too long, though with hindsight, I should have taken my camel pack!
Whoa, where are you going with this?
I trained: averaged 12mph for the first set and 9mpg for the second. On that evidence, 100 miles is going to take me 9hrs. Not a bad stab but I really want to do the ride in 8hours (with 30 minutes of breaks).
That’s an average of 12.5mph no matter the gradient and I suspect there’ll be some big hills out there. It’s not East Anglia after all.
One of the things I’d really like to do by June is be able to ride from Felixstowe to Cambridge 71 miles. I’m working up to that slowly.
Last year I went from 10miles to 47miles in seven weeks.
I’ve kept a base fitness up over the winter, but two months out after getting a bad stomach bug. So six months should allow me to do that easily.
Week 1 (this week): 1 ride of 25 miles and 1 ride of 10 miles. Some hill training. A day off in between.
Week 2 (w/c 25th Feb): 1 ride 35 miles and 1 ride of 10 miles. 30 minutes hill training.
Week 3 (w/c 4th Mar): 1 ride 35 miles (different route) and 1 ride of 10 miles. 45 minutes hill training (I have a route).
Week 4 (w/c 11th Mar): 1 ride of 25 miles, looking at how close I get can to 2hours and 1 ride of 10 miles aiming for an hour max. 60 mins hill training. A day off in between.
This is important as that’s an average of 12.5mph regardless of local gradient. The 21st Feb, I am significantly under that.
Week 5 (w/c 18th Mar): 1 ride of 40 miles and 1 ride of 15 miles. 20 mins hill training. A day off in between.
Week 6 (w/c 25th Mar): 1 ride 40 miles and 1 ride of 15 miles. 20 minutes hill training.
Week 7 (w/c 1st Apr): 1 ride 40 miles and 1 ride of 10 miles. 60 minutes hill training.
Week 8 (w/c 8th Apr): 1 ride of 40 miles, looking at how close I get can to 3hours. This is likely to be to Woolpit along route 51.
Week 9 (w/c 15 Apr): 1 ride 50 miles (aiming for 5 hours), 2 sets of hill training. Possibly up the A137.
Week 10 (w/c 22 Apr): 1 ride 50 miles (aiming for 4.5 hours). Gym work and 2 sets of hill training.
Week 11 (w/c 29 Apr): 1 ride 50 miles (aiming for 4 hours). Gym work and 2 sets of hill training.
Week 12 (w/c 6 May): 1 ride 50 miles (aiming for 3.5 hours). Gym work and 2 sets of hill training.
Week 13 (w/c 13 May): 1 ride 60 miles (aiming for 5 hours) (average 12mph), 2 sets of hill training.
Week 14 (w/c 20 May): 1 ride 60 miles (aiming for 5 hours). Gym work and 2 sets of hill training.
Week 15 (w/c 27 May): 1 ride 60 miles (aiming for 4.5 hours). Gym work and 2 sets of hill training.
Week 16 (w/c 3 Jun): 1 ride 60 miles (aiming for 4 hours). Gym work and 2 sets of hill training. Probably Felixstowe to Newmarket.
Week 17 (w/c 10 Jun): Week off. Just walking and motorcycling.
Week 18 (w/c 17 Jun): 1 ride 70 miles (aiming for 6 hours). Gym work and 2 sets of hill training.
Week 19 (w/c 24 Jun): 1 ride 70 miles. Gym work and 2 sets of hill training.
Week 20 (w/c 1 Jul): 1 ride 80 miles (aiming for 7 hours).
Week 21 (w/c 8 Jul): 1 ride 90 miles (aiming for 8 hours).
Week 22 (w/c 15 Jul) : 1 ride 90 miles (aiming for 7 hours).
Week 23 (w/c 22 Jul): 1 ride 100 miles (aiming for 8 hours).
Week 24 (w/c 29 Jul): Hill training, 2 sets, 10 mins each.
Ride the ride 4th August.
Posted: February 21st, 2019 under 42, Prudential ride 2019.
Comments: none